

全美最大医院运营商HCA蒸蒸日上,当地人却想把它赶出城外
ERIKA FRY
2022-04-07
HCA公司在疫情期间创下利润新高。但该公司最近收购的一家医疗集团的病人和医护人员却表示,财务回报和服务质量毫无关系。
 文本设置
文本设置
 Plus(0条)
Plus(0条) 

2020年2月,小威尔·奥弗费尔特在父亲床边陪侍了将近两个礼拜。那时,他父亲刚刚被诊断出癌症晚期,住进了Mission医院,这家医院位于阿什维尔市中心,有815张床位。奥弗费尔特是当地教育系统的行为分析员,一直很为这家医院感到自豪,因为它经常被评为全美顶级医院,而正是因为这里的优质医疗服务,他才劝说自己年迈体弱的父母从家乡弗吉尼亚州来到了北卡罗来纳州。
但是奥弗费尔特的医院陪护经历让他非常不满。医院里从病房到电梯在内的所有设施都脏兮兮的,而且人手严重短缺,感觉无法保障病人的安全:当他因为父亲疼痛难忍或弄脏了床单按呼叫铃时,永远没有人来。最后他总是不得不去走廊里四处寻找工作人员。入院的第一天,他父亲把一张用过的纸巾掉在了床边的地板上。之后的日子里,奥弗费尔特路过时总会看一眼那张纸还在不在,以此来判断有没有人来打扫过房间。他们在那住了近两个礼拜,那张纸一动也没动。
想到在父亲最后的生命里,会有一段时间在这里度过,他感到十分痛苦。他意识到,他们只是这家大医院里的其中一个家庭,他想,这种事是不是会发生在每个人身上呢?
为了回答这个问题,今年44岁自称“超级内向”的奥弗费尔特做了个“石蕊实验”:他在Facebook上创建了一个小组,提出了这个问题。他原以为会有10到15个人报名,但等他第二天早上登陆网站时,发现申请加入这个私人小组的有几百人。每天都继续有很多新人加入,其中很大一部分会在入群后分享自己在Mission医院的痛苦经历——人手短缺、天价账单、护理问题等等。
我们中有许多人在我们自己的医院里却无法得到细心照料,也无法感到安全。
小威尔·奥弗费尔特
在奥弗费尔特以及聚在他的Facebook群组中的大多数人看来,这些问题的罪魁祸首毫无争议:美国最大的盈利性医院运营商HCA Healthcare公司。Mission医院原本是一个以社区为基础的非营利性医院,但在经营了133年之后,包括该医院及5家小型乡村医院在内的Mission Health集团被HCA收购了。这笔交易价值15亿美元,完成于2019年2月。该协议得到了这家医疗集团董事会的一致支持,阿什维尔的这些精英们认为这笔交易可以最大化地保障Mission Health的未来,同时提升本地社区的卫健水平。这笔收益将用于建立一个规模宏大的地区卫生基金会——以人均资金计算,是全国同类基金会中规模最大的——而且,与Mission不同的是,HCA可以通过纳税为当地注入更多资金。
但公众并不买账。阿什维尔是一个有着强烈的购买本地商品情结的山城,由营利性企业经营Mission集团的新闻立刻引发了关注和怀疑。Mission集团旗下的乡村医院可以辐射18个相距甚远的周边县区,在这些地区看来,这笔交易意味着背叛。董事会认为,这笔交易可以确保Mission有一个长久健康的未来;但在许多公众眼中,这相当于给Mission判了死刑。
然后疫情爆发了。
过去两年,新冠肺炎疫情就像美国医疗行业的破城槌,带来一个又一个考验,不断损耗着全美医疗体系:患者激增、供应受限、营业中断、劳动力短缺、员工疲惫不堪等等。
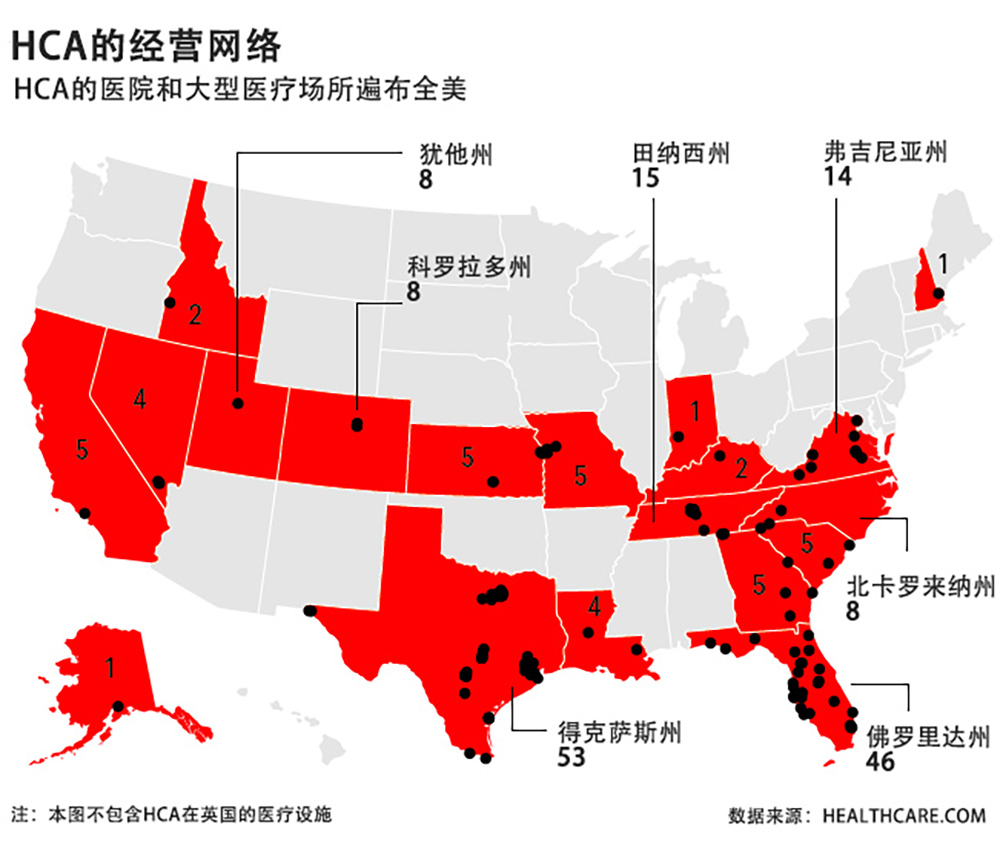
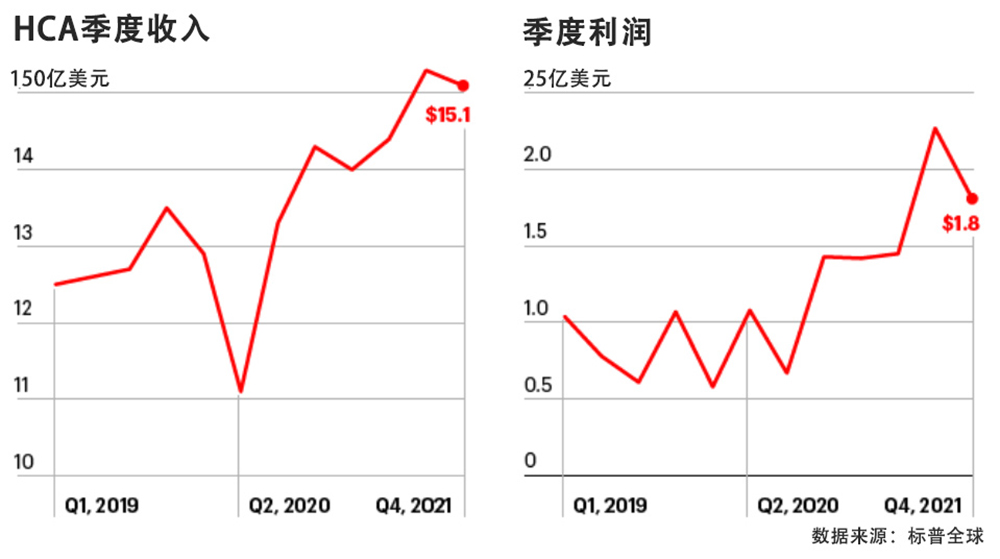
HCA一直处于这一切的中心;全美没有哪家医疗集团比HCA收治的新冠病患更多了 (到2021年共26万名)。然而,这家在全美拥有180多家医院的公司却在2021年大获成功,营收和利润分别达到了创纪录的588亿美元和70亿美元。甚至在2020年,即使因为被要求暂停利润较高的择期手术导致HCA的盈利大受打击,该公司的利润仍比2019年增长了7%。这些数字还不包括该公司向联邦政府返还了60亿美元的《新冠病毒援助、救济与经济安全法案》(CARES Act,旨在新冠肺炎疫情期间为医院提供支持)补贴。而且,自疫情爆发以来,HCA在资本项目上投资了64亿美元,投资87亿美元用于股票回购,还给公司首席执行官山姆•黑森发了约1.17亿美元(包括已股份和期权)。
SVB Leerink的高级研究分析师惠特•梅奥称,该公司的业绩十分出色:“HCA拥有医院行业目前最优秀的经营人才,这点毫无疑问。”
在Mission向当地提交的最新报告中,HCA北卡罗来纳州总裁格雷格·劳写道,因为Mission手头有了新的企业资源,疫情期间应对十分出色。他说,与许多同行不同,HCA没有因为疫情让员工停薪留职,而在资源短缺的时候,因为公司规模足够大,可以向需求急切的地区调拨资源。格雷格称,Mission因此而受益,其安全等级被评为行业最高的A级,比前两年要高,医院的护理水平也得到了高度认可。他强调,HCA将继续对Mission集团进行投资,包括在富兰克林农村建一所新医院,以及在阿什维尔建一座当地亟需的行为健康医疗机构。
但Mission医院的病人说,他们不认可格雷格所描述的这副蒸蒸日上的场景。Mission流失了数百名员工,留下来的工作人员总说人手不够,工作环境不可持续。当地人称Mission农村医院的医疗服务遭到了削减。北卡罗来纳州总检察长办公室已经收到了数以百计的关于HCA的投诉,账单问题、护理质量、人员配备、清洁问题等等,不一而足,当地媒体也多次就同样的问题进行过报道。
与此同时,奥弗费尔特的Facebook群组已经发展到将近13000名成员,他们把这里当成了布告栏,分享自己糟糕的医疗经历(偶尔也有一些正面评价),对美国医疗体系的现状进行讨论。奥弗费尔特和其他五名公民对Mission和HCA提起了反垄断诉讼,指控他们在北卡罗来纳州搞垄断。(针对奥弗费尔特的就医经历,HCA北卡罗来纳州分部的发言人南希·林德尔回应道,病患的不满意,“总是让我们感到失望”,但她补充说,医院一直在提供优质护理。)
为撰写本文,《财富》杂志采访了几十位病人、护士、医生、当地领导人、华尔街分析师和学者。(HCA拒绝让高管接受采访。)采访出现了两种截然不同、难以融合的观点。北卡罗来纳州有许多人强烈认为HCA毁了Mission。另一些人则严重怀疑,如果Mission必须靠自己应对疫情,它现在会是什么样子。
“有各种各样的说法和解释。“保罗·凯克里说,他是一名资深医疗顾问,在阿什维尔和纳什维尔两地工作,他也对这件事感到困惑。“每一种说法你都能听到一点。”
HCA收购Mission Health的故事非常特别,但也揭示了美国医院加大合力度这一现象背后残酷的经济原理。这个行业利润微薄,而业界只有愿意削减成本、扩大规模和追逐利润的机构才能获得财务回报,这一点不是疫情造成的,却因为疫情而加剧。问题是:我们的卫生系统因为前所未有的疫情压力屈服,那么全美规模最大的医院运营商是如何脱颖而出、大获全胜的?如果HCA的胜利告诉人们什么是“有效”的做法,那对医疗行业的未来意味着什么?
阿什维尔给人的感觉可能是一个热闹的时髦中心,但环绕这座城市的蓝岭山脉无时无刻不在提醒着人们,它是通往阿巴拉契亚的门户,连接的是北卡罗来纳西端以农村为主的多个郡县。这个地区曾经是切诺基民族的一部分,吸引着丹尼尔·布恩这样的拓荒者,也是乔治·范德比尔特这样的富人后代的乡村游乐场;如今,这座拥有9万人口的城市逐渐成为越来越多艺术家、美食家和想要拥有高品质医疗的退休人士的目的地。
对于生活在北卡州西部的近100万居民来说,Mission是个家喻户晓的名字。这是当地最重要的医疗集团,拥有最全面的创伤治疗服务和最综合的医疗护理。因此,对于当地许多人来说,HCA可能要收购Mission的消息令他们十分震惊。“我做梦也想不到会是HCA,”史蒂夫·诺斯医生说,他曾在北卡罗来纳州农村山地松(Spruce Pine)地区担任Mission的地区医疗主任。
在一些人看来,Mission和HCA之间的根本区别可以追溯到它们各自的起点。Mission的历史起源于19世纪末,当地4名妇女走上街头卖花,想要筹集资金建一家愿意收治所有人的医院,无论病人有没有钱付医药费。这个后来被称为“小花传教会”(The Little Flower Mission)的组织在一座租来的房子里开业了,于1885年10月接待了第一位病人——一名产妇。
HCA也起源于一座房子,但相似之处也仅限于此。HCA成立于1968年,由弗里斯特家族的两位内科医生——28岁的小汤米和他父亲老托马斯(老托马斯的另一个医生儿子比尔后来成为了参议院多数党领袖)以及他们开肯德基的商人朋友杰克·梅西共同成立。他们三个想把肯德基的成功配方——标准化和规模化——带到私立医院。HCA这个名字说明了一切: Hospital Corporation of America,美国医院公司。
HCA经历过几次迭代,最近一次始于2011年,当时正值美国准备通过《平价医疗法案》(Affordable Care Act)扩大医保覆盖范围,它进行了公司历史上的第三次上市。自那以后,HCA的股价上涨了738%,营收几乎翻了一番,从307亿美元增至590亿美元。
这么长时间里,HCA从未真正偏离其最初的配方:规模。“他们的运作非常高效……他们在采购物资时会进行有力谈判;他们会保持较低的员工成本,”凯克利说。他们还会把床位填得很满,入住率超过70%。
如今,HCA的业务覆盖43个市场。该公司在选址上讲究策略,往往选择经济活跃、快速发展的地区,也就是拥有私人医疗保险的富人愿意居住的地区。与使用医疗保险(Medicare)或医疗补助(Medicaid)的患者相比,这类患者会给医疗服务提供商支付更高的费用。HCA进入一个新地区后,会建立一个高密度护理网络,包括独立的急诊,急救中心、手术中心等。
该公司另一个增长战略是吸引“高敏度”患者,也就是病情较重或者需要更复杂的治疗护理服务的患者。这些患者同样意味着更多钱。为了吸引这类患者,HCA加大了对创伤中心、新生儿重症监护室和中风中心等类似设施的投资。
尽管HCA的营生处于无法预测的生死之间,该公司却以数据驱动和专注于目标而闻名。(疫情打断了HCA住院率连续23个季度的增长。)“HCA是应试教学。”凯克里说,“为了达到优化股东价值所需要的质量或效率水平,他们会考到所需要的那个分数。”
从这个角度来看,北卡西部似乎是一个糟糕的投资。比该州其他地方相比,这个地区的人们更老、更穷、病情更严重,Mission近四分之三的病人都有医疗保险、医疗补助,或者根本没有医保。约翰·鲍尔说,被HCA收购之前,Mission收治的大部分病例都是亏钱的,鲍尔是Mission前高管,出售Mission时是集团的董事会主席。
Mission需要改变算法,这也是在出售前的几年里,集团首席执行官罗恩•保卢斯一直的努力方向。保卢斯曾是一名医生,后来凭借沃顿商学院(Wharton)的打磨成为医院高管。他于2010年来到阿什维尔,当时许多人认为,美国价值2.6万亿美元已经失控的医疗体系即将迎来革命性的变化。
变革的动力是一种被称为“基于价值的医疗”理念,而保卢斯正是来自于少数几个成功实施了这一理念的机构之一——宾夕法尼亚州的盖辛格健康中心(Geisinger Health),他是这种理念的拥护者。该理念希望把这个治病救人的行业变成保健行业,奥巴马时代的医疗政策也源自于此。实施此战略需要在预防医学和初级保健等领域加大投资,从而确保及早发现问题,避免患者发展到需要昂贵复杂治疗的阶段。还需要一种新的商业模式:从为医疗提供者的服务付费转为“为效果付费“。
保卢斯向该模式投入了大量资金,到2015年,Mission拥有了一个由8家医院和1100名初级保健医生组成的网络,为当地提供基于价值的医疗服务。只有医保患者才有资格享受相关服务,但在最初几年,实验取得了成功,交出了高质量的答卷,为Mission带来了500万美元。
保卢斯的计划奏效了,但还不够快。雄心勃勃的扩张削减了Mission的营业利润。领导层本希望通过向商业保险患者收取更高费用来抵消成本,但2017年,该集团的主要付款方——北卡罗来纳州的蓝十字和蓝盾协会(Blue Cross and Blue Shield of North Carolina)拒绝提高保险费率,计划破灭了。
鲍尔回忆说:“当时,所有看起来唾手可及的成果都被砍掉了。”他说,就只剩下一些极端的选项:关闭医院和业务线,裁掉1400个工作岗位。董事会否掉了这个选择,决定寻找一个买家。
将Mission出售给HCA或许无论如何都不是件易事。但董事会的沟通策略无异于火上浇油。当地人甚至不知道Mission准备出售了,更没有机会在HCA已经成为潜在买主前发表意见建议。尽管保卢斯和鲍尔在公开场合兜售他们眼中这笔交易的最大卖点:HCA的购买力、税收,以及成立一个专注于社区医疗的价值15亿美元的基金会,但这还是让人们产生了怀疑、愤愤不平。
在北卡罗来纳州的总检察长审查这笔交易时,关心此事的居民们积极活动,想要争取更有力的保护条款,他们实现了目标。最终的购买协议要求HCA保证Mission的五家乡村医院继续开放,一些服务项目要维持至少10年。
对于那些见证了以价值为基础的医疗变革成功的人来说,随后看到的是痛苦的解体。虽然该项目没有被立刻枪毙,但“当时的态度是,初级保健不再是真正重要的业务,”曾在Mission工作的医生诺斯说。他曾为多名物质滥用障碍病人提供治疗,当HCA与在初级保健业务中提供必要支持的治疗师们解除合同时,他离开了,集团里9位医生领头人中除了两位,其他人也都离开了。HCA的林德尔说,该系统目前正在加大其对基于价值的医疗服务的承诺。
对于HCA来说,Mission的交易是公司剧本中的全新一章。通常情况下,该公司的收购对象是陷入紧急财务困境的医院。但是,正如HCA的高管们所述,Mission是一个“独特的成功的医疗集团”,是一个“示范性”收购案例,他们希望这个案例能帮他们争取到与其他经营状况良好的大型医院系统的交易。
鲍尔说,上述目标让Mission董事会相信,HCA不会“把事情搞砸”,但事后看来,这笔交易中的新情况似乎让HCA对抵制毫无准备。“在其他地方,他们的到来拯救了一家医院,所以当地人欢迎他们。他们对于进入一个不欢迎他们的社区没什么经验。”
HCA标志性的精益运营模式却没有在实践中得到认可。该公司的第一个重大变革是取消了Mission系统中的健康单元协调员。长期以来,健康单元协调员在医院里承担着维持秩序的重要角色——接听电话、跟踪医嘱、将信息传递给正确的人。取消这个职位成功砍掉了医院许多部门,却带来了混乱。工作人员不得不从看护工作中抽身接电话。“这件事意义重大,”安吉拉·福斯特说。她从2013年到2020年底在Mission担任行政助理,直到她自己的岗位(以及医院翻译和一些牧师职位)被取消。“这是最先对病人护理和员工满意度产生真正负面影响的事件之一。”林德尔表示,这一变革“原意是为了加强临床护理”,她还说,HCA后来撤销了这条政策,当年就恢复了协调员的岗位。
护士们还告诉我,在HCA将医院的餐饮服务和清洁工作外包后,她们常常不得不自己送餐、倾倒垃圾桶。与此同时,人员变化也给他们带来了更大压力。2016年,当克里·威尔逊开始在阿什维尔医院的心脏病观察科室工作时,该科室共有13名护士,5名助理护士、2名协调员和2名遥测技术员一起工作,科室处于满员状态。威尔逊说,HCA接手后,同样的工作量由11名护士、4名助理护士、1名协调员和1名技术员承担。(她说,由于劳动力短缺,该科室经常人手不足)。
至少对于Mission集团中其中一家较为偏远的医院来说,HCA的到来似乎威胁到了自身的存亡。拥有25张床位的特兰西瓦尼亚地区医院位于布里瓦德镇,这个8000人口的小镇毗邻皮斯加国家森林,位于阿什维尔西南45分钟车程。与许多乡村医院一样,特兰西瓦尼亚医院近年来遇上了财务困难(Mission在2015年关闭了它的分娩科),这类医院主要为穷人和老年人服务,否则他们就得长途跋涉才能看上病。即使HCA在收购协议中加入了保护条款,当地仍有许多人对它的未来忧心忡忡。
12月初,我约见了布里瓦德市长莫林·科佩洛夫。这是她正式上任的第一天,但她位于市政厅的办公室看起来已经准备就绪,墙上挂着照片,办公桌上整整齐齐地放着成摞的文件。市政厅是主街上一栋低矮的小建筑。
科佩洛夫任职前是市议会成员,那时她就已经陷入了与HCA的纷纷扰扰之中。2021年1月,HCA与特兰西瓦尼亚医院的医生重新商签合同,想要将工资改为更低的绩效制,导致该医院大部分医生集体离职。尽管人们提出,其他工资模式可能更适合农村医院,留住经验丰富的医生对医院来说很有必要,但该公司丝毫不为所动。
“他们有一份标准合同,”科佩洛夫说,声音里透着恼怒。“想要根据我们当地的需求来定制的想法根本不可能实现。”
HCA坚称,它对当地拥有的每一家医疗场所都进行了投资。该公司称,它正向特兰西瓦尼亚医院投入1400万美元,包括购置一台新的MRI机器、修建一座直升机停机坪。林德尔表示,公司在让特兰西瓦尼亚医院为“爆炸性人口增长”做好准备,而科佩洛夫和其他人看到的却是医院的服务正在缓慢而安静地受到侵蚀。

科佩洛夫说,问题在于,什么才是购买协议中承诺的“提供”服务。这家医院的工作人员和病患说,医院每周提供服务和预约的天数减少了,每天工作的时间也减少了。需要经济援助进行非紧急治疗的患者
只有在他们的慈善医疗获批后才能看病,而这个批准过程十分官僚,有时甚至需要Mission的首席医务官签字。
还有人说,医院已经脱离了社区。“这只是一种不同的企业文化,”布里瓦德的皮斯加健康基金会(Pisgah Health Foundation)主席莱克斯•格林表示。格林在2020年初建了一个“得来速”式新冠病毒检测站,当时隔壁县的帕迪(Pardee)医院派出了首席执行官、一名流行病学专家和一名社区外展服务人员来帮忙。而HCA对格林的回应基本上是:“我们不提供免费检测。”(林德尔指出,该医院2020年缴纳了6000万美元的州和地方税。)
格林多年来一直为Mission筹款,也是本次出售计划的啦啦队长。他认为该公司承诺成立的15亿美元的基金会可以改变这个社区,而且他有和HCA接触的一些经验:他的孩子是在该公司佛罗里达州的一家医院出生的。
但后来他有了在HCA经营下的Mission医院看病的第一次经历。去年夏天,他已故的母亲,一位老年痴呆患者住进了Mission医院。医院人手非常紧张,他说他母亲有时都吃不上饭。他回忆说,一次探病时,一名护士告诉他,“我们没办法保证全部医嘱都能落实到位。我们实在是太忙了。”又一天,她母亲换了病房。工作人员把他领到六楼的一个房间,结果房间里却是一个陌生人。工作人员向他道歉,说他的母亲实际上正在做手术。他被吓到了,呆坐在那里。后来再去打听,才发现原来母亲并没有在做手术,而是被换到了七楼的一个房间。
“HCA是应试教学。为了达到优化股东价值所需要的质量或效率水平,他们会考到需要的那个分数。句号。”
保罗·凯克里,资深医疗咨询师
格林不确定Mission医疗服务水平的倒退在多大程度上是因为疫情,但他说这种医院环境“是个悲剧”。他的家人认为这也加剧了他母亲的病重。
这样的故事我听过很多,它们描述了在HCA运营下的Mission提供的医疗服务混乱不堪,甚至无法确保病人的安全。有个女士的化验样本丢了。还有很多人不得不长时间坐在自己的排泄物里,在走廊或手术间的床上躺上好几个小时。坦率而充满歉意的护士跟他们说:“我们人手不足。”
心脏病观察科室的那个护士威尔逊说,她们科室一直在努力防止病人摔倒(这种情况通常发生在病人想在没有护士的情况下自己上厕所时),以及防止病人在弄脏的床上坐太久引发的皮肤问题。尽管她已经尽力了,但仍时常觉得自己辜负了病人。
林德尔强调,提供高质量的医疗服务是Mission的首要任务,他通过引用该集团收获的最高评级和积极反馈来力证其成功。在与患者沟通时,HCA将这些糟糕的经历归咎于疫情以及全国范围内的大规模医护短缺。很难计算Mission的人手问题应该在多大程度上归咎于疫情,又在多大程度上是由新老板造成的人员流失导致的。当然,疫情对劳动力市场的负面影响是雪上加霜:HCA目前总共为Mission Health集团放出了1080个岗位空缺。林德尔说,公司正在努力填补缺口。
在我采访过的护士里,有人离开Mission是因为环境,也有人是因为她们有机会当旅行护士,拿现在三倍高的薪水。和其他医院一样,HCA自己也开始雇用“旅行护士”以解决人手短缺问题,而这种方案显然并不完美:旅行护士通常不熟悉当地的医疗体系和病人,而他们的薪酬却比熟悉这些的人高得多。(Mission员工说,本院部分部门七成以上员工都是旅行护士。)
他们对于进入一个不欢迎他们的社区没什么经验。”
约翰·鲍尔,Mission前高管,出售Mission时任董事会主席
分析人士说,HCA因为有护理学校和人力资源公司,在应对人手短缺问题时比大多数公司都做得好。而且尽管人手短缺,该公司的利润率仍然比疫情前要高,分析人士认为,部分原因是该公司为应对疫情快速进行了成本重组。瑞穗(Mizuho)美洲区高级分析师安•海因斯说,该公司的市场分布也帮了忙。德克萨斯州和佛罗里达州是HCA最大的两个市场,这两个市场很快就重新开放了,管控政策也不那么严格,经营环境接近于正常。
与直觉相反,疫情在某些方面还提升了HCA的利润。纵观整个行业,去医院的人变少了。但那些去医院的人往往可能有商业保险(因为老年医保患者都呆在家里),而且病情更严重(要么是得了新冠,要么是被耽误的其他疾病)。虽然照顾新冠患者的成本很高,但联邦政府会向医疗机构额外支付20%的费用,所以利润也更高;HCA收治了最多新冠肺炎患者的一个季度也是其业绩最好的几个季度之一(不过海因斯将其业绩归因于整体的入院率高)。
美国银行(Bank of America)分析师凯文·费施贝克说:“与HCA和广大医院的主要争论点在于,新冠对他们的影响到底是积极的还是消极的?”如果没有政府出资支撑其利润率,答案几乎肯定是否定的。SVB Leerink分析师梅奥怀疑,这些钱最终是否会被收回:“有些公司业绩非常非常好。联邦政府会在在某个时候开始批评这种做法。”
对于医疗行业而言,以病人为中心的使命和利润驱动的使命永远都存在尴尬的紧张关系。作为美国最大的盈利性医院运营商,HCA很容易被当成坏人,尽管专家说事情并没有那么简单。在一个著名的医院指数中,HCA在薪酬公平和价值方面的评价很差,但临床结果的评价很高。
在收益电话会议上,HCA对此次收购做出了积极评价。收购后的第一年,该公司将价格提高了10%,病人总收入比非营利性的Mission在收购前一年的收入多出5.49亿美元。
但围绕Mission的戏剧性事件似乎远未解决。奥弗费尔特说:“我们中有许多人在我们自己的医院里却无法得到细心照料,也无法感到安全。”他每周仍花15到20个小时维系Facebook上的Mission群组。
虽然HCA对报道中许多更具争议性的观点提出了异议,但该公司在实践中却默认了患者存在不满的现实。HCA北卡罗来纳州分部的总裁劳将他的个人电话号码提供给了每一个遇上账单问题的人。
HCA在阿什维尔的工作仍在继续。他们近期的关注点是“吞吐量”——尽可能高效地为病人办理入院出院。威尔逊正在适应医院的出院流程,包括将病人送到出院套房,撤掉床上用品以及清理房间。环境服务团队的预算是花30分钟来打扫房间。
威尔逊说,“如果他们能把我们变成一条装配线,他们会这么做的。”
美国国立卫生研究院基金会(NIHCM Foundation)的捐款为本篇报道提供了支持。(财富中文网)
本文发表于《财富》杂志2022年4月/ 5月刊,标题为《利润与损失》("Profit and loss")。
译者:Agatha
2019年,阿什维尔最大的医疗机构Mission医院被HCA收购,一同被收购的还有5家社区医院,共计15亿美元。照片来源:杰里米·M·兰格
2020年2月,小威尔·奥弗费尔特在父亲床边陪侍了将近两个礼拜。那时,他父亲刚刚被诊断出癌症晚期,住进了Mission医院,这家医院位于阿什维尔市中心,有815张床位。奥弗费尔特是当地教育系统的行为分析员,一直很为这家医院感到自豪,因为它经常被评为全美顶级医院,而正是因为这里的优质医疗服务,他才劝说自己年迈体弱的父母从家乡弗吉尼亚州来到了北卡罗来纳州。
但是奥弗费尔特的医院陪护经历让他非常不满。医院里从病房到电梯在内的所有设施都脏兮兮的,而且人手严重短缺,感觉无法保障病人的安全:当他因为父亲疼痛难忍或弄脏了床单按呼叫铃时,永远没有人来。最后他总是不得不去走廊里四处寻找工作人员。入院的第一天,他父亲把一张用过的纸巾掉在了床边的地板上。之后的日子里,奥弗费尔特路过时总会看一眼那张纸还在不在,以此来判断有没有人来打扫过房间。他们在那住了近两个礼拜,那张纸一动也没动。
想到在父亲最后的生命里,会有一段时间在这里度过,他感到十分痛苦。他意识到,他们只是这家大医院里的其中一个家庭,他想,这种事是不是会发生在每个人身上呢?
为了回答这个问题,今年44岁自称“超级内向”的奥弗费尔特做了个“石蕊实验”:他在Facebook上创建了一个小组,提出了这个问题。他原以为会有10到15个人报名,但等他第二天早上登陆网站时,发现申请加入这个私人小组的有几百人。每天都继续有很多新人加入,其中很大一部分会在入群后分享自己在Mission医院的痛苦经历——人手短缺、天价账单、护理问题等等。
我们中有许多人在我们自己的医院里却无法得到细心照料,也无法感到安全。
小威尔·奥弗费尔特
在奥弗费尔特以及聚在他的Facebook群组中的大多数人看来,这些问题的罪魁祸首毫无争议:美国最大的盈利性医院运营商HCA Healthcare公司。Mission医院原本是一个以社区为基础的非营利性医院,但在经营了133年之后,包括该医院及5家小型乡村医院在内的Mission Health集团被HCA收购了。这笔交易价值15亿美元,完成于2019年2月。该协议得到了这家医疗集团董事会的一致支持,阿什维尔的这些精英们认为这笔交易可以最大化地保障Mission Health的未来,同时提升本地社区的卫健水平。这笔收益将用于建立一个规模宏大的地区卫生基金会——以人均资金计算,是全国同类基金会中规模最大的——而且,与Mission不同的是,HCA可以通过纳税为当地注入更多资金。
但公众并不买账。阿什维尔是一个有着强烈的购买本地商品情结的山城,由营利性企业经营Mission集团的新闻立刻引发了关注和怀疑。Mission集团旗下的乡村医院可以辐射18个相距甚远的周边县区,在这些地区看来,这笔交易意味着背叛。董事会认为,这笔交易可以确保Mission有一个长久健康的未来;但在许多公众眼中,这相当于给Mission判了死刑。
然后疫情爆发了。
过去两年,新冠肺炎疫情就像美国医疗行业的破城槌,带来一个又一个考验,不断损耗着全美医疗体系:患者激增、供应受限、营业中断、劳动力短缺、员工疲惫不堪等等。
HCA一直处于这一切的中心;全美没有哪家医疗集团比HCA收治的新冠病患更多了 (到2021年共26万名)。然而,这家在全美拥有180多家医院的公司却在2021年大获成功,营收和利润分别达到了创纪录的588亿美元和70亿美元。甚至在2020年,即使因为被要求暂停利润较高的择期手术导致HCA的盈利大受打击,该公司的利润仍比2019年增长了7%。这些数字还不包括该公司向联邦政府返还了60亿美元的《新冠病毒援助、救济与经济安全法案》(CARES Act,旨在新冠肺炎疫情期间为医院提供支持)补贴。而且,自疫情爆发以来,HCA在资本项目上投资了64亿美元,投资87亿美元用于股票回购,还给公司首席执行官山姆•黑森发了约1.17亿美元(包括已股份和期权)。
SVB Leerink的高级研究分析师惠特•梅奥称,该公司的业绩十分出色:“HCA拥有医院行业目前最优秀的经营人才,这点毫无疑问。”
在Mission向当地提交的最新报告中,HCA北卡罗来纳州总裁格雷格·劳写道,因为Mission手头有了新的企业资源,疫情期间应对十分出色。他说,与许多同行不同,HCA没有因为疫情让员工停薪留职,而在资源短缺的时候,因为公司规模足够大,可以向需求急切的地区调拨资源。格雷格称,Mission因此而受益,其安全等级被评为行业最高的A级,比前两年要高,医院的护理水平也得到了高度认可。他强调,HCA将继续对Mission集团进行投资,包括在富兰克林农村建一所新医院,以及在阿什维尔建一座当地亟需的行为健康医疗机构。
但Mission医院的病人说,他们不认可格雷格所描述的这副蒸蒸日上的场景。Mission流失了数百名员工,留下来的工作人员总说人手不够,工作环境不可持续。当地人称Mission农村医院的医疗服务遭到了削减。北卡罗来纳州总检察长办公室已经收到了数以百计的关于HCA的投诉,账单问题、护理质量、人员配备、清洁问题等等,不一而足,当地媒体也多次就同样的问题进行过报道。
与此同时,奥弗费尔特的Facebook群组已经发展到将近13000名成员,他们把这里当成了布告栏,分享自己糟糕的医疗经历(偶尔也有一些正面评价),对美国医疗体系的现状进行讨论。奥弗费尔特和其他五名公民对Mission和HCA提起了反垄断诉讼,指控他们在北卡罗来纳州搞垄断。(针对奥弗费尔特的就医经历,HCA北卡罗来纳州分部的发言人南希·林德尔回应道,病患的不满意,“总是让我们感到失望”,但她补充说,医院一直在提供优质护理。)
为撰写本文,《财富》杂志采访了几十位病人、护士、医生、当地领导人、华尔街分析师和学者。(HCA拒绝让高管接受采访。)采访出现了两种截然不同、难以融合的观点。北卡罗来纳州有许多人强烈认为HCA毁了Mission。另一些人则严重怀疑,如果Mission必须靠自己应对疫情,它现在会是什么样子。
“有各种各样的说法和解释。“保罗·凯克里说,他是一名资深医疗顾问,在阿什维尔和纳什维尔两地工作,他也对这件事感到困惑。“每一种说法你都能听到一点。”
HCA收购Mission Health的故事非常特别,但也揭示了美国医院加大合力度这一现象背后残酷的经济原理。这个行业利润微薄,而业界只有愿意削减成本、扩大规模和追逐利润的机构才能获得财务回报,这一点不是疫情造成的,却因为疫情而加剧。问题是:我们的卫生系统因为前所未有的疫情压力屈服,那么全美规模最大的医院运营商是如何脱颖而出、大获全胜的?如果HCA的胜利告诉人们什么是“有效”的做法,那对医疗行业的未来意味着什么?
阿什维尔给人的感觉可能是一个热闹的时髦中心,但环绕这座城市的蓝岭山脉无时无刻不在提醒着人们,它是通往阿巴拉契亚的门户,连接的是北卡罗来纳西端以农村为主的多个郡县。这个地区曾经是切诺基民族的一部分,吸引着丹尼尔·布恩这样的拓荒者,也是乔治·范德比尔特这样的富人后代的乡村游乐场;如今,这座拥有9万人口的城市逐渐成为越来越多艺术家、美食家和想要拥有高品质医疗的退休人士的目的地。
对于生活在北卡州西部的近100万居民来说,Mission是个家喻户晓的名字。这是当地最重要的医疗集团,拥有最全面的创伤治疗服务和最综合的医疗护理。因此,对于当地许多人来说,HCA可能要收购Mission的消息令他们十分震惊。“我做梦也想不到会是HCA,”史蒂夫·诺斯医生说,他曾在北卡罗来纳州农村山地松(Spruce Pine)地区担任Mission的地区医疗主任。
在一些人看来,Mission和HCA之间的根本区别可以追溯到它们各自的起点。Mission的历史起源于19世纪末,当地4名妇女走上街头卖花,想要筹集资金建一家愿意收治所有人的医院,无论病人有没有钱付医药费。这个后来被称为“小花传教会”(The Little Flower Mission)的组织在一座租来的房子里开业了,于1885年10月接待了第一位病人——一名产妇。
HCA也起源于一座房子,但相似之处也仅限于此。HCA成立于1968年,由弗里斯特家族的两位内科医生——28岁的小汤米和他父亲老托马斯(老托马斯的另一个医生儿子比尔后来成为了参议院多数党领袖)以及他们开肯德基的商人朋友杰克·梅西共同成立。他们三个想把肯德基的成功配方——标准化和规模化——带到私立医院。HCA这个名字说明了一切: Hospital Corporation of America,美国医院公司。
小威尔·奥弗费尔特对父亲在Mission医院的住院经历感到愤怒,因此在Facebook上创建了一个小组,以这个医疗集团为讨论话题;这个小组现在有将近13000名成员。照片来源:杰里米·M·兰格
HCA经历过几次迭代,最近一次始于2011年,当时正值美国准备通过《平价医疗法案》(Affordable Care Act)扩大医保覆盖范围,它进行了公司历史上的第三次上市。自那以后,HCA的股价上涨了738%,营收几乎翻了一番,从307亿美元增至590亿美元。
这么长时间里,HCA从未真正偏离其最初的配方:规模。“他们的运作非常高效……他们在采购物资时会进行有力谈判;他们会保持较低的员工成本,”凯克利说。他们还会把床位填得很满,入住率超过70%。
如今,HCA的业务覆盖43个市场。该公司在选址上讲究策略,往往选择经济活跃、快速发展的地区,也就是拥有私人医疗保险的富人愿意居住的地区。与使用医疗保险(Medicare)或医疗补助(Medicaid)的患者相比,这类患者会给医疗服务提供商支付更高的费用。HCA进入一个新地区后,会建立一个高密度护理网络,包括独立的急诊,急救中心、手术中心等。
该公司另一个增长战略是吸引“高敏度”患者,也就是病情较重或者需要更复杂的治疗护理服务的患者。这些患者同样意味着更多钱。为了吸引这类患者,HCA加大了对创伤中心、新生儿重症监护室和中风中心等类似设施的投资。
尽管HCA的营生处于无法预测的生死之间,该公司却以数据驱动和专注于目标而闻名。(疫情打断了HCA住院率连续23个季度的增长。)“HCA是应试教学。”凯克里说,“为了达到优化股东价值所需要的质量或效率水平,他们会考到所需要的那个分数。”
从这个角度来看,北卡西部似乎是一个糟糕的投资。比该州其他地方相比,这个地区的人们更老、更穷、病情更严重,Mission近四分之三的病人都有医疗保险、医疗补助,或者根本没有医保。约翰·鲍尔说,被HCA收购之前,Mission收治的大部分病例都是亏钱的,鲍尔是Mission前高管,出售Mission时是集团的董事会主席。
Mission需要改变算法,这也是在出售前的几年里,集团首席执行官罗恩•保卢斯一直的努力方向。保卢斯曾是一名医生,后来凭借沃顿商学院(Wharton)的打磨成为医院高管。他于2010年来到阿什维尔,当时许多人认为,美国价值2.6万亿美元已经失控的医疗体系即将迎来革命性的变化。
变革的动力是一种被称为“基于价值的医疗”理念,而保卢斯正是来自于少数几个成功实施了这一理念的机构之一——宾夕法尼亚州的盖辛格健康中心(Geisinger Health),他是这种理念的拥护者。该理念希望把这个治病救人的行业变成保健行业,奥巴马时代的医疗政策也源自于此。实施此战略需要在预防医学和初级保健等领域加大投资,从而确保及早发现问题,避免患者发展到需要昂贵复杂治疗的阶段。还需要一种新的商业模式:从为医疗提供者的服务付费转为“为效果付费“。
尽管当地的农村居民担心HCA会削减服务,但该公司正在北卡罗来纳州人口只有4000的富兰克林镇建设天使医疗中心(Angel Medical Center)照片来源:杰里米·M·兰格
保卢斯向该模式投入了大量资金,到2015年,Mission拥有了一个由8家医院和1100名初级保健医生组成的网络,为当地提供基于价值的医疗服务。只有医保患者才有资格享受相关服务,但在最初几年,实验取得了成功,交出了高质量的答卷,为Mission带来了500万美元。
保卢斯的计划奏效了,但还不够快。雄心勃勃的扩张削减了Mission的营业利润。领导层本希望通过向商业保险患者收取更高费用来抵消成本,但2017年,该集团的主要付款方——北卡罗来纳州的蓝十字和蓝盾协会(Blue Cross and Blue Shield of North Carolina)拒绝提高保险费率,计划破灭了。
鲍尔回忆说:“当时,所有看起来唾手可及的成果都被砍掉了。”他说,就只剩下一些极端的选项:关闭医院和业务线,裁掉1400个工作岗位。董事会否掉了这个选择,决定寻找一个买家。
将Mission出售给HCA或许无论如何都不是件易事。但董事会的沟通策略无异于火上浇油。当地人甚至不知道Mission准备出售了,更没有机会在HCA已经成为潜在买主前发表意见建议。尽管保卢斯和鲍尔在公开场合兜售他们眼中这笔交易的最大卖点:HCA的购买力、税收,以及成立一个专注于社区医疗的价值15亿美元的基金会,但这还是让人们产生了怀疑、愤愤不平。
在北卡罗来纳州的总检察长审查这笔交易时,关心此事的居民们积极活动,想要争取更有力的保护条款,他们实现了目标。最终的购买协议要求HCA保证Mission的五家乡村医院继续开放,一些服务项目要维持至少10年。
对于那些见证了以价值为基础的医疗变革成功的人来说,随后看到的是痛苦的解体。虽然该项目没有被立刻枪毙,但“当时的态度是,初级保健不再是真正重要的业务,”曾在Mission工作的医生诺斯说。他曾为多名物质滥用障碍病人提供治疗,当HCA与在初级保健业务中提供必要支持的治疗师们解除合同时,他离开了,集团里9位医生领头人中除了两位,其他人也都离开了。HCA的林德尔说,该系统目前正在加大其对基于价值的医疗服务的承诺。
对于HCA来说,Mission的交易是公司剧本中的全新一章。通常情况下,该公司的收购对象是陷入紧急财务困境的医院。但是,正如HCA的高管们所述,Mission是一个“独特的成功的医疗集团”,是一个“示范性”收购案例,他们希望这个案例能帮他们争取到与其他经营状况良好的大型医院系统的交易。
鲍尔说,上述目标让Mission董事会相信,HCA不会“把事情搞砸”,但事后看来,这笔交易中的新情况似乎让HCA对抵制毫无准备。“在其他地方,他们的到来拯救了一家医院,所以当地人欢迎他们。他们对于进入一个不欢迎他们的社区没什么经验。”
HCA标志性的精益运营模式却没有在实践中得到认可。该公司的第一个重大变革是取消了Mission系统中的健康单元协调员。长期以来,健康单元协调员在医院里承担着维持秩序的重要角色——接听电话、跟踪医嘱、将信息传递给正确的人。取消这个职位成功砍掉了医院许多部门,却带来了混乱。工作人员不得不从看护工作中抽身接电话。“这件事意义重大,”安吉拉·福斯特说。她从2013年到2020年底在Mission担任行政助理,直到她自己的岗位(以及医院翻译和一些牧师职位)被取消。“这是最先对病人护理和员工满意度产生真正负面影响的事件之一。”林德尔表示,这一变革“原意是为了加强临床护理”,她还说,HCA后来撤销了这条政策,当年就恢复了协调员的岗位。
护士们还告诉我,在HCA将医院的餐饮服务和清洁工作外包后,她们常常不得不自己送餐、倾倒垃圾桶。与此同时,人员变化也给他们带来了更大压力。2016年,当克里·威尔逊开始在阿什维尔医院的心脏病观察科室工作时,该科室共有13名护士,5名助理护士、2名协调员和2名遥测技术员一起工作,科室处于满员状态。威尔逊说,HCA接手后,同样的工作量由11名护士、4名助理护士、1名协调员和1名技术员承担。(她说,由于劳动力短缺,该科室经常人手不足)。
至少对于Mission集团中其中一家较为偏远的医院来说,HCA的到来似乎威胁到了自身的存亡。拥有25张床位的特兰西瓦尼亚地区医院位于布里瓦德镇,这个8000人口的小镇毗邻皮斯加国家森林,位于阿什维尔西南45分钟车程。与许多乡村医院一样,特兰西瓦尼亚医院近年来遇上了财务困难(Mission在2015年关闭了它的分娩科),这类医院主要为穷人和老年人服务,否则他们就得长途跋涉才能看上病。即使HCA在收购协议中加入了保护条款,当地仍有许多人对它的未来忧心忡忡。
布里瓦德的市长莫林·科佩洛夫说,她试图说服HCA根据本地社区的实际需求开展业务,但这种努力“没有希望成功”。照片来源:杰里米·M·兰格
12月初,我约见了布里瓦德市长莫林·科佩洛夫。这是她正式上任的第一天,但她位于市政厅的办公室看起来已经准备就绪,墙上挂着照片,办公桌上整整齐齐地放着成摞的文件。市政厅是主街上一栋低矮的小建筑。
科佩洛夫任职前是市议会成员,那时她就已经陷入了与HCA的纷纷扰扰之中。2021年1月,HCA与特兰西瓦尼亚医院的医生重新商签合同,想要将工资改为更低的绩效制,导致该医院大部分医生集体离职。尽管人们提出,其他工资模式可能更适合农村医院,留住经验丰富的医生对医院来说很有必要,但该公司丝毫不为所动。
“他们有一份标准合同,”科佩洛夫说,声音里透着恼怒。“想要根据我们当地的需求来定制的想法根本不可能实现。”
HCA坚称,它对当地拥有的每一家医疗场所都进行了投资。该公司称,它正向特兰西瓦尼亚医院投入1400万美元,包括购置一台新的MRI机器、修建一座直升机停机坪。林德尔表示,公司在让特兰西瓦尼亚医院为“爆炸性人口增长”做好准备,而科佩洛夫和其他人看到的却是医院的服务正在缓慢而安静地受到侵蚀。
科佩洛夫说,问题在于,什么才是购买协议中承诺的“提供”服务。这家医院的工作人员和病患说,医院每周提供服务和预约的天数减少了,每天工作的时间也减少了。需要经济援助进行非紧急治疗的患者
只有在他们的慈善医疗获批后才能看病,而这个批准过程十分官僚,有时甚至需要Mission的首席医务官签字。
还有人说,医院已经脱离了社区。“这只是一种不同的企业文化,”布里瓦德的皮斯加健康基金会(Pisgah Health Foundation)主席莱克斯•格林表示。格林在2020年初建了一个“得来速”式新冠病毒检测站,当时隔壁县的帕迪(Pardee)医院派出了首席执行官、一名流行病学专家和一名社区外展服务人员来帮忙。而HCA对格林的回应基本上是:“我们不提供免费检测。”(林德尔指出,该医院2020年缴纳了6000万美元的州和地方税。)
格林多年来一直为Mission筹款,也是本次出售计划的啦啦队长。他认为该公司承诺成立的15亿美元的基金会可以改变这个社区,而且他有和HCA接触的一些经验:他的孩子是在该公司佛罗里达州的一家医院出生的。
但后来他有了在HCA经营下的Mission医院看病的第一次经历。去年夏天,他已故的母亲,一位老年痴呆患者住进了Mission医院。医院人手非常紧张,他说他母亲有时都吃不上饭。他回忆说,一次探病时,一名护士告诉他,“我们没办法保证全部医嘱都能落实到位。我们实在是太忙了。”又一天,她母亲换了病房。工作人员把他领到六楼的一个房间,结果房间里却是一个陌生人。工作人员向他道歉,说他的母亲实际上正在做手术。他被吓到了,呆坐在那里。后来再去打听,才发现原来母亲并没有在做手术,而是被换到了七楼的一个房间。
“HCA是应试教学。为了达到优化股东价值所需要的质量或效率水平,他们会考到需要的那个分数。句号。”
保罗·凯克里,资深医疗咨询师
格林不确定Mission医疗服务水平的倒退在多大程度上是因为疫情,但他说这种医院环境“是个悲剧”。他的家人认为这也加剧了他母亲的病重。
这样的故事我听过很多,它们描述了在HCA运营下的Mission提供的医疗服务混乱不堪,甚至无法确保病人的安全。有个女士的化验样本丢了。还有很多人不得不长时间坐在自己的排泄物里,在走廊或手术间的床上躺上好几个小时。坦率而充满歉意的护士跟他们说:“我们人手不足。”
心脏病观察科室的那个护士威尔逊说,她们科室一直在努力防止病人摔倒(这种情况通常发生在病人想在没有护士的情况下自己上厕所时),以及防止病人在弄脏的床上坐太久引发的皮肤问题。尽管她已经尽力了,但仍时常觉得自己辜负了病人。
林德尔强调,提供高质量的医疗服务是Mission的首要任务,他通过引用该集团收获的最高评级和积极反馈来力证其成功。在与患者沟通时,HCA将这些糟糕的经历归咎于疫情以及全国范围内的大规模医护短缺。很难计算Mission的人手问题应该在多大程度上归咎于疫情,又在多大程度上是由新老板造成的人员流失导致的。当然,疫情对劳动力市场的负面影响是雪上加霜:HCA目前总共为Mission Health集团放出了1080个岗位空缺。林德尔说,公司正在努力填补缺口。
在我采访过的护士里,有人离开Mission是因为环境,也有人是因为她们有机会当旅行护士,拿现在三倍高的薪水。和其他医院一样,HCA自己也开始雇用“旅行护士”以解决人手短缺问题,而这种方案显然并不完美:旅行护士通常不熟悉当地的医疗体系和病人,而他们的薪酬却比熟悉这些的人高得多。(Mission员工说,本院部分部门七成以上员工都是旅行护士。)
他们对于进入一个不欢迎他们的社区没什么经验。”
约翰·鲍尔,Mission前高管,出售Mission时任董事会主席
分析人士说,HCA因为有护理学校和人力资源公司,在应对人手短缺问题时比大多数公司都做得好。而且尽管人手短缺,该公司的利润率仍然比疫情前要高,分析人士认为,部分原因是该公司为应对疫情快速进行了成本重组。瑞穗(Mizuho)美洲区高级分析师安•海因斯说,该公司的市场分布也帮了忙。德克萨斯州和佛罗里达州是HCA最大的两个市场,这两个市场很快就重新开放了,管控政策也不那么严格,经营环境接近于正常。
与直觉相反,疫情在某些方面还提升了HCA的利润。纵观整个行业,去医院的人变少了。但那些去医院的人往往可能有商业保险(因为老年医保患者都呆在家里),而且病情更严重(要么是得了新冠,要么是被耽误的其他疾病)。虽然照顾新冠患者的成本很高,但联邦政府会向医疗机构额外支付20%的费用,所以利润也更高;HCA收治了最多新冠肺炎患者的一个季度也是其业绩最好的几个季度之一(不过海因斯将其业绩归因于整体的入院率高)。
美国银行(Bank of America)分析师凯文·费施贝克说:“与HCA和广大医院的主要争论点在于,新冠对他们的影响到底是积极的还是消极的?”如果没有政府出资支撑其利润率,答案几乎肯定是否定的。SVB Leerink分析师梅奥怀疑,这些钱最终是否会被收回:“有些公司业绩非常非常好。联邦政府会在在某个时候开始批评这种做法。”
对于医疗行业而言,以病人为中心的使命和利润驱动的使命永远都存在尴尬的紧张关系。作为美国最大的盈利性医院运营商,HCA很容易被当成坏人,尽管专家说事情并没有那么简单。在一个著名的医院指数中,HCA在薪酬公平和价值方面的评价很差,但临床结果的评价很高。
在收益电话会议上,HCA对此次收购做出了积极评价。收购后的第一年,该公司将价格提高了10%,病人总收入比非营利性的Mission在收购前一年的收入多出5.49亿美元。
但围绕Mission的戏剧性事件似乎远未解决。奥弗费尔特说:“我们中有许多人在我们自己的医院里却无法得到细心照料,也无法感到安全。”他每周仍花15到20个小时维系Facebook上的Mission群组。
虽然HCA对报道中许多更具争议性的观点提出了异议,但该公司在实践中却默认了患者存在不满的现实。HCA北卡罗来纳州分部的总裁劳将他的个人电话号码提供给了每一个遇上账单问题的人。
HCA在阿什维尔的工作仍在继续。他们近期的关注点是“吞吐量”——尽可能高效地为病人办理入院出院。威尔逊正在适应医院的出院流程,包括将病人送到出院套房,撤掉床上用品以及清理房间。环境服务团队的预算是花30分钟来打扫房间。
威尔逊说,“如果他们能把我们变成一条装配线,他们会这么做的。”
美国国立卫生研究院基金会(NIHCM Foundation)的捐款为本篇报道提供了支持。(财富中文网)
本文发表于《财富》杂志2022年4月/ 5月刊,标题为《利润与损失》("Profit and loss")。
译者:Agatha
Will Overfelt Jr. spent nearly two weeks of February 2020 at his father’s bedside. His father had just been diagnosed with terminal cancer and admitted to Mission Hospital, an 815-bed facility in downtown Asheville. Overfelt, who works as a behavior analyst for the local school system, had long held a sense of pride in the institution—it’s often ranked as a top hospital—and he had lured his ailing parents to Western North Carolina from his native Virginia in part because of the quality health care there.
But Overfelt’s time inside the hospital, keeping watch over his dying dad, was deeply upsetting. He found the facilities, from the room to the elevators, to be filthy, and the place felt so understaffed as to be unsafe for patients: When he rang the call bell, because his father was in ferocious pain, or because he had soiled the bed, no one came. Eventually, he’d wander the halls, looking for staff. The first day there, his father dropped a used tissue that landed on the floor, near the edge of the bed. In his comings and goings, Overfelt would check whether the tissue was still there as a sort of gauge—did anyone ever clean the room?—and, over the nearly two-week stay, it never budged.
It pained him that this is where his father would spend some of his final days. He realized his was one family in a very large hospital, but he wondered, Is this happening to everyone?
As a sort of “litmus test,” Overfelt, who is 44 and a self-described “super-introvert,” created a Facebook group and put the question out there. He had expected to hear from 10 or 15 people, but when he checked the site the next morning, requests to join the private group numbered in the hundreds. Every day there were more, many from people who would then post their own distressing experiences—understaffing, nightmare billing, care issues—at the hospital.
Many of us don't feel cared for or safe in our hospital anymore.
WILL OVERFELT JR.
To Overfelt, and the many amassing in his Facebook group, there was little question as to whom to blame for the problems: HCA Healthcare, the nation’s largest for-profit hospital operator. After 133 years operating as a community-based nonprofit, Mission Health, the hospital system that included Mission Hospital, as well as five smaller rural facilities, had recently been bought by HCA. The $1.5 billion sale went through in February 2019. It had been unanimously backed by Mission’s board, a roster of Asheville elite who championed the deal as the best way to ensure Mission’s future and improve health in the community. The proceeds would be used to create an enormous regional health foundation—the largest of its kind in the country, in dollars per capita—and HCA, unlike Mission, would pump more money into the area by paying taxes.
The broader public wasn’t convinced. In Asheville, a mountain town with strong buy-local vibes, the prospect of a corporate operator drew immediate concern and suspicion. In the surrounding, often remote 18-county area served by Mission’s rural hospitals, it registered as a betrayal. The board believed it was securing for Mission a long, healthy future; many in the public felt it had given it a death sentence.
Then the pandemic hit.
Over the past two years, COVID-19 has been the battering ram at the gates of American health care, wearing down the system, one test after the next: patient surges, constrained supplies, business disruptions, labor shortages, worker burnout—on and on.
HCA has been at the center of it all; no U.S. health system has treated more COVID inpatients (a total of 260,000 through 2021). Yet the company, with its more than 180 hospitals across the country, had a blockbuster 2021, posting record revenues and profits: $58.8 billion and $7 billion, respectively. Not even 2020, a year when hospitals were required to suspend profit-generating elective procedures, hit HCA's books particularly hard: Profits were up 7% over 2019. And those figures were after the company returned $6 billion in CARES Act funding—money intended to shore up hospitals during COVID—to the federal government. Since the pandemic began, HCA also invested $6.4 billion on capital projects, spent $8.7 billion on stock buybacks and paid its CEO, Sam Hazen, roughly $117 million (including vested stock and realized options).
Whit Mayo, a senior research analyst with SVB Leerink, called the company's performance remarkable. "Inside HCA, by far, you have the best operating talent in the hospital industry," he says. "No question."
In Mission’s most recent report to the community, HCA North Carolina president Greg Lowe wrote that Mission capably navigated the pandemic thanks to the new corporate resources at its disposal. Unlike many of its peers, HCA did not furlough workers due to the pandemic, and at moments of scarcity, the company’s scale allowed it to distribute resources where needed, he said. That benefited Mission, which Lowe noted was awarded the industry’s top A safety grade—an improvement over the two previous years—and earned recognition for its nursing program. He emphasized that HCA continues to invest in Mission, which includes building a new hospital in rural Franklin and a much-needed behavioral health facility in Asheville.
But many Mission patients say they don’t recognize the thriving hospital system Lowe describes. Mission has lost hundreds of employees, and those who remain speak of understaffed and unsustainable conditions. Community members contend services have been reduced at Mission’s rural hospitals. The office of North Carolina’s attorney general has received hundreds of complaints concerning HCA’s practices, from billing to quality of care to staffing and cleanliness, subjects that have also been doggedly reported by local press.
Overfelt’s Facebook group, meanwhile, has grown to nearly 13,000 members who use the site as a bulletin board for bad experiences, a few positive ones, and general discussion of American health care. He, along with five other citizens, has filed an antitrust suit against Mission and HCA, alleging that the N.C. system is a monopoly. (In response to Overfelt’s experience, Nancy Lindell, a spokesperson for HCA’s North Carolina division, says “we’re always disappointed” when patients have a negative experience, but adds that the hospital continues to deliver quality care.)
Fortune spoke with dozens of people—patients, nurses, doctors, local leaders, Wall Street analysts, and academics—for this story. (HCA declined to make executives available for interviews.) It’s difficult to reconcile the two vastly different pictures that emerge. Many people in North Carolina feel passionately that HCA has ruined Mission. Others seriously wonder in what shape Mission would be had it had to manage the pandemic on its own.
“It’s all anecdotal. It’s all spin,” says Paul Keckley, a longtime health care consultant who splits his time between Asheville and Nashville, and is himself puzzled by the case. “You hear a little bit of everything.”
The saga of HCA’s acquisition of Mission Health is a highly specific but also revealing story about the brutal economics that underpin the U.S.’s increasingly consolidated hospital landscape. COVID didn’t create the industry’s razor-thin margins, or make it a field in which the financial rewards flow only to those willing to cut costs, amass scale, and chase profits, but it has exacerbated the situation. It also raises questions: After our health system bowed under the unprecedented strain of the pandemic, how is it that the country’s biggest hospital player has emerged such a winner? And if HCA is a sign of what “works,” what does that mean for the future of care?
Asheville may feel like a buzzy, progressive center, but the Blue Ridge Mountains that ring the city are an ever-present reminder that it’s the gateway to Appalachia and the mostly rural counties that make up North Carolina’s western tip. Once part of the Cherokee nation, the region was a draw for frontiersmen like Daniel Boone and a country playground for wealthy scions such as George Vanderbilt; today, the city of 90,000 is an increasingly crowded destination for artists, foodies, and health-care-conscious retirees.
For the nearly 1 million living in Western North Carolina, Mission is a household name. It’s the region’s dominant health system, with the most comprehensive trauma services and complex medical care. So for many in the community the news of Mission’s prospective buyer came as a shock. “Never in my wildest dreams would I have guessed HCA,” says Steve North, a physician who served as Mission’s regional medical director in rural Spruce Pine, N.C.
What some see as the fundamental divide between Mission and HCA can be traced all the way back to their origin stories. Mission’s roots date to the late 1800s, when four local women began selling flowers on the street to raise funds for a hospital that would treat all, regardless of their ability to pay. “The Little Flower Mission,” as the group came to be known, operated out of a rented house and served its first patient, a woman in labor, in October 1885.
HCA was also started out of a house, but the similarities end there. Founded in 1968, HCA was launched by two physicians in the Frist family—28-year-old Tommy Jr. and his father, Thomas Sr. (another of Thomas Sr.’s doctor sons, Bill, would go on to become Senate majority leader)—along with their businessman friend, Jack Massey, an owner of Kentucky Fried Chicken. The trio wanted to bring the same formula of standardization and scale that had powered the success of KFC to private hospitals. The name said it all: HCA, for Hospital Corporation of America.
Upset by the care his father received at Mission, Will Overfelt Jr. started a Facebook group to discuss the hospital system; it now has almost 13,000 members.
HCA has been though several iterations, but the latest began in 2011, when it went public for the third time in its history as the nation prepared for the expansion of insurance coverage through the Affordable Care Act. Since then, HCA’s stock has risen 738%, and its revenues nearly doubled, from $30.7 billion to $59 billion.
In all that time, HCA never really strayed from its original recipe: scale. “They operate very efficiently ... They’re going to procure their supplies with aggressive negotiations; they’re going to keep their staffing costs low,” says Keckley. The company keeps beds filled as well, with occupancy rates above 70%.
Today, HCA operates in 43 markets. The company is strategic about its locations, selecting fast-growing areas with vibrant economies, the sort where affluent people with private health insurance tend to live. (Providers are paid significantly higher rates for those patients, compared to those with Medicare or Medicaid.) When it moves into an area, HCA builds out a dense network of care sites—including freestanding emergency departments, as well as urgent care and surgery centers.
Another aspect of the company’s growth strategy is to draw “higher acuity” patients—those who are sicker or in need of more complex medical care. Those patients represent more money, too, and the pursuit of them has driven HCA’s investment in things like trauma centers, neonatal intensive care units, and stroke centers.
Despite operating in the unpredictable realm of life and death, HCA is famously data-driven and consistently on-target. (It took a pandemic to end its 23-quarter streak of increased admission rates.) “HCA teaches to the test,” says Keckley. “They will hit the number necessary to hit the level of quality or efficiency that optimizes their shareholder value. Period.”
From that point of view, Western North Carolina seems like a bad bet. Older, poorer, and sicker than elsewhere in the state, nearly three-quarters of Mission’s patients have Medicare, Medicaid, or no insurance coverage at all. Pre-HCA, Mission actually lost money on most of its patients, says John Ball, a former hospital executive who chaired Mission’s board at the time of the sale.
The system needed to change the math, and in the years before the sale, that’s what CEO Ron Paulus tried to do. Paulus, a physician turned hospital executive with Wharton polish, arrived in Asheville in 2010 at a moment when many believed America’s runaway, then– $2.6 trillion health system was poised for revolutionary change.
The engine of that change was something called “value-based care,” and Paulus, who hailed from one of the few places that had successfully implemented it—Pennsylvania’s Geisinger Health—was a believer. The idea, which animated Obama-era health policies, was to pivot an industry focused on treating sick people to one that aims to keep people healthy. It’s a strategy that requires investment in areas like preventive medicine and primary care, with the goal of catching problems early, before patients need costly, complicated care. It also demands a new business model: paying providers not for the services they perform, but for successful outcomes.
While rural communities fear HCA will cut services, the company is currently building Angel Medical Center in the 4,000-person town of Franklin, N.C.
Paulus plowed money into the model, and by 2015, Mission had a network of eight hospitals and 1,100 primary care physicians providing value-based care in the region. Only Medicare patients were eligible, but in its first years, the experiment was successful, delivering high quality scores and a $5 million payment to Mission.
Paulus’s plan was working, but not fast enough. The ambitious expansion cut into Mission’s operating margins. Leadership wanted to offset costs by charging patients with commercial insurance more—a strategy that the system’s major payer, Blue Cross and Blue Shield of North Carolina, crushed when it refused to raise rates in 2017.
“We’d gotten to the point where all of the low-hanging fruit have been cut,” recalls Ball. That left drastic options, he says: ultimately closing hospitals and lines of service, and cutting 1,400 jobs. The board decided, instead, to find a buyer.
The sale of Mission to HCA was probably never going to be an easy process. But the board’s communication strategy didn’t do it any favors. Locals didn’t even know Mission was up for sale, let alone have the chance to offer input before HCA emerged as the likely buyer. That made people distrusting and resentful even as Paulus and Ball publicly pushed what they considered the deal’s biggest selling points: HCA's purchasing power, tax revenue, and the creation of a $1.5 billion foundation focused on community health.
As North Carolina’s attorney general reviewed the sale, concerned citizens campaigned for stronger protections and got them—leading to a final purchase agreement that requires HCA to keep open Mission’s five rural hospitals and provide certain services for at least 10 years.
For those who had witnessed the success of the value-based care efforts, a painful dismantling followed. Though the program wasn’t killed outright, “There was an attitude primary care was no longer really important,” North, the former Mission doctor, says. He treated a number of patients with substance abuse disorders, and when HCA terminated contracts with therapists who provided essential support to the primary care efforts, he left, as have all but two of system’s nine physician leaders. HCA’s Lindell says the system is currently expanding its commitment to value-based care.
For HCA, the Mission deal represented a new chapter in its playbook. Typically, the company acquired hospitals in urgent financial distress. But Mission, as HCA executives described it, was a “uniquely successful system,” a “showcase” acquisition that they hoped would help them court other deals involving large, well-run hospital systems.
Those ambitions gave the Mission board confidence the company wouldn’t “screw this up,” says Ball, but in hindsight, they also created a new dynamic, seemingly leaving HCA unprepared for pushback. “In every other place, they’ve come in and rescued a hospital, and the community liked them. They didn’t have a lot of experience with coming in and having a community not like them.”
HCA’s signature lean operating model was not well received on the ground. One of company’s first big changes was to eliminate many of the system’s health unit coordinators, or HUCs. The HUCs had long played a vital, order-keeping role at the hospital—answering phones, tracking orders, communicating messages to the right people. Getting rid of them effectively decapitated many units of the hospital, unleashing chaos. Staff were now pulled from care to pick up phones. “That was a really big deal,” says Angela Foster, who worked at Mission as an administrative assistant from 2013 until late 2020 when her own job was eliminated (along with hospital translators and some chaplains). “It was one of the first things that had a real detrimental effect to patient care and to staff satisfaction.” Lindell says the change was “meant to bolster clinical care” and noted that the company walked back the change, reinstating HUCs later that year.
Nurses also told me they often ended up delivering food and emptying trash bins after HCA outsourced the hospital’s food service and janitorial functions. Meanwhile, staffing changes piled more on them, too. When Kerri Wilson started working at the Asheville hospital’s cardiac step-down unit in 2016, she was one of 13 nurses who worked with a team of five nursing assistants (CNAs), two HUCs, and two telemetry techs when the unit was fully staffed. Under HCA, Wilson says the same patient load is covered by 11 nurses, four CNAs, one HUC, and one off-site telemetry tech. (She says that because of the labor shortage, the unit is often not fully staffed.)
For at least one of Mission’s more remote hospitals, the arrival of HCA felt like an existential threat. The system’s 25-bed Transylvania Regional Hospital (TRH) is based in Brevard, a town of 8,000 that borders the Pisgah National Forest, 45 minutes southwest of Asheville. Like many rural hospitals that serve the typically poorer and older populations that would otherwise have to travel a long distance for care, TRH had struggled financially in recent years (Mission shuttered its labor and delivery unit in 2015). Even with the protections of HCA’s purchase agreement, many in the community worried for its future.
Brevard's mayor, Maureen Copelof, says attempts to persuade HCA to work around the needs of her community have been a "nonstarter."
JEREMY M. LANGE
I met with Brevard’s mayor, Maureen Copelof, in early December. It was her first official day in the job, but her office at City Hall, a small, squat building on Main Street, looked fully settled, with framed photographs on the walls and stacks of papers arranged neatly on her desk.
And as a former city council member, Copelof was already enmeshed in the HCA saga. In January 2021, the majority of TRH’s physicians left their jobs en masse when HCA tried to renegotiate their contracts with lower, performance- based pay rates. The company was unmoved by arguments that a different pay model may be better suited to rural areas or that there’s a value in holding on to experienced physicians.
“They have a standard contract,” Copelof said, exasperation in her voice. “The idea of trying to tailor something to meet the needs of our community—it was a nonstarter.”
HCA insists it’s investing in all its regional facilities. At TRH it points to $14 million in improvements, including a new MRI machine and a paved helipad. But while Lindell says the company is preparing TRH for “explosive population growth,” Copelof and others see a slow, quiet erosion of services.
The question, says Copelof, is what counts as “providing” service, as promised in the purchase agreement. People who use and work in the hospital say services and appointments are available fewer days of the week, and fewer hours per day. Patients who need financial assistance for nonemergency treatment can’t be seen until their charity care is approved, a bureaucratic process that in some cases requires sign-off from Mission’s chief medical officer.
Others say the hospital has disengaged with the community. “It’s just a different corporate culture,” says Lex Green, president of Brevard’s Pisgah Health Foundation. When he set up a drive-thru COVID testing site in early 2020, Pardee, the hospital in the neighboring county, sent its CEO, an epidemiologist, and a community outreach person to help. HCA’s response to Green was, essentially, “We do not provide free tests.” (Lindell notes that the hospital paid $60 million in state and local taxes in 2020.)
Green, who spent years as a fundraiser for Mission, had been a cheerleader for the sale. He thought the $1.5 billion foundation it created could transform the community—and he’d had some previous experience with HCA: His children were born at one of the company’s Florida hospitals.
But then he had his first experience with HCA-run Mission. Last summer, his late mother, a dementia patient, was admitted to Mission Hospital. Staffing was so stretched that he says his mother went unfed at times. On one visit, he recalls a nurse telling him, “There is no way we can ensure all the doctor’s orders are going to be done. We’re just too busy here.” Another day, she’d been moved. A staff member directed him to a room on the sixth floor where he found a stranger. The staff member apologized and told him, actually his mother was in surgery. He sat in shock, before asking again. It turned out his mom was not in surgery, but in a room on the seventh floor.
“HCA teaches to the test. They will hit the level of quality or efficiency that optimizes their shareholder value. Period.”
PAUL KECKLEY, A LONGTIME HEALTH CARE CONSULTANT
Green is not sure how much the pandemic factored into that failing care, but he describes the hospital conditions as “tragic.” His family members believe it contributed to his mother’s decline.
His was one of numerous stories I heard that paint a picture of chaotic and at times unsafe care at Mission under HCA. There was a woman whose lab specimen got lost. There were multiple people who had to sit for long periods in their own feces or were kept for hours on a bed in a hallway or operating bay. Many had been told by frank and apologetic nurses, “We’re understaffed.”
Wilson, the cardiac step-down nurse, says her unit has struggled to prevent patient falls—an event that typically happens when, absent a nurse, people try to get to the toilet on their own—and the skin issues that arise when patients have been sitting too long in a soiled bed. She often feels, despite doing her best, that she is failing her patients.
Lindell emphasizes that quality care is the system’s top priority, and cites the system’s top ratings and positive feedback it receives as evidence that it’s succeeding. In communications with patients, HCA places such experiences in the context of COVID and the broader, nationwide shortage of health care workers. It’s hard to know how much of Mission’s staffing woes to blame on the pandemic versus attrition driven by new ownership. Certainly COVID’s disruption of the labor market has not helped: HCA currently lists 1,080 job openings in the Mission Health system. Lindell says the company is working diligently to fill them.
I spoke to nurses who left Mission because of the environment, but also because of the opportunity to get paid at least three times as much to work as a travel nurse. And like other hospital companies, HCA has itself turned to “travelers,” an imperfect staffing solution: They’re often unfamiliar with local systems and patients, and they get paid way more than those who are. (Some Mission units have been staffed by more than 70% travelers, say employees.)
“HCA didn't have a lot of experience with coming in and having a community not like them.”
JOHN BALL, A FORMER HOSPITAL EXECUTIVE WHO CHAIRED MISSION’S BOARD AT THE TIME OF THE SALE
Analysts say HCA, which owns nursing schools and a staffing firm, has managed the labor challenges better than most. And despite the issue, the company’s margins are higher than they were pre-pandemic, which analysts in part credit to its swift cost restructuring in response to COVID. The company’s geography also helped, says Mizuho Americas senior analyst Ann Hynes. Texas and Florida, HCA’s largest markets, reopened quickly and had generally less restrictive policies, making for a closer-to-normal operating environment.
Counterintuitively, some aspects of the pandemic actually made HCA even more profitable. Across the industry, fewer people have been going to the hospital. But those who have, have been more likely to be commercially insured (because older Medicare patients are staying home) and to be sicker (either with COVID or because of delayed treatment for some other condition). While caring for COVID patients is expensive, the federal government pays providers an additional 20%, making those cases more profitable than they would otherwise be for HCA; one of the company’s strongest quarters was also the one where had its highest level of COVID patients (though Hynes attributes the results to high admission rates generally).
“The big debate with HCA and hospitals broadly speaking,” says Bank of America analyst Kevin Fischbeck, “is has COVID been a positive or a negative?” Had government money not propped up margins, the answer would almost certainly be no. Mayo, the SVB Leerink analyst, wonders if some of that money might eventually be clawed back: “There are companies that have done very, very well. At some point, the federal government is going to begin to criticize this.”
The business of health care will always have awkward tension around the patient-centered mission and the profit-driven one. As the nation’s largest for-profit hospital operator, HCA is an easy villain, though experts say it’s not that simple. On one prominent hospital index, HCA rates poorly on pay equity and value, but quite well when it comes to clinical outcomes.
On earnings calls, HCA discusses the acquisition in positive terms. In its first year, the company raised prices 10% and took in $549 million more in gross patient revenues than not-for-profit Mission had in the year before the acquisition.
But the drama that surrounds Mission feels far from resolved. “Many of us don’t feel cared for or safe in our hospital anymore,” says Overfelt, who still spends 15 to 20 hours a week tending the Mission Facebook group.
While HCA disputed many of the more contentious points raised in this reporting, the company does show a tacit awareness of discontent. Lowe, the N.C. division president, made his personal phone number available to anyone experiencing billing issues.
In Asheville, the company’s work continues. These days, there’s an emphasis on “throughput”—getting the patients in and out of the hospital as efficiently as possible. Wilson is adjusting to the hospital’s discharge protocols, which involve sending the patient to the discharge suite, stripping the bed, and clearing the room. The environmental services team is budgeted 30 minutes for cleaning the room.
Says nurse Wilson, “If they could turn us into an assembly line, they would.”
A grant from the NIHCM Foundation helped fund reporting for this story.
This article appears in the April/May 2022 issue of Fortune with the headline, "Profit and loss."
请打开财富Plus APP